TO THE EDITOR:Coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome (SARS) coronavirus 2, was initially identified in the city of Wuhan, capital of the Hubei province of China, in December of 2019. (1) On March 11, 2020, the World Health Organization characterized the disease as a pandemic.(2) As of April 26, there were approximately 3 million confirmed cases of COVID-19 and 206,000 deaths attributed to the disease worldwide. The highest numbers of confirmed cases were in the United States (n = 963,379) and Spain (n = 226,629), whereas the highest numbers of deaths were in Italy (n = 26,644) and France (n = 23,190).(3)
In Brazil, the first COVID-19 case was confirmed on February 26, 2020, in the city of São Paulo. On March 17, the first death from the disease was reported in the country. On April 24, Brazil already ranked 11th worldwide in terms of the number of confirmed cases (n = 52,995) and the number of deaths (n = 3,670).(4)
Given the continental dimensions of Brazil and its internal economic, social, and cultural inequalities, the impact of the disease might be heterogeneous. Therefore, the objective of the present study was to analyze the spatiotemporal distribution of case fatality rates (CFRs) of COVID-19 in the 26 Brazilian states and the Federal District of Brasília (all hereafter referred to as states) between epidemiological week (EW) 12 and EW 17 of 2020 (from March 17 to April 24).
This was an ecological study of all deaths due to COVID-19, by state and EW. Data were obtained from the Brazilian National Ministry of Health (https://covid.saude.gov.br/) on April 24, 2020. The CFRs for each state and EW were then calculated. The CFR is defined as the proportion of deaths from a given disease in relation to the total number of patients with that disease:

An exploratory spatiotemporal analysis was conducted, and choropleth maps were prepared in order to show the results. Because only secondary, public-domain data were used in the present study, the requirement for approval by the local research ethics committee was waived.
Between EW 9 and EW 17, Brazil reported 52,995 cases of COVID-19 and 3,670 deaths, with a CFR of 6.9%. The first deaths were reported on March 17 (in EW 12) in the states of Rio de Janeiro (n = 3) and São Paulo (n = 15), which subsequently accounted for 2,082 (56.7%) of the COVID-19-related deaths in the country during the period studied (Figure 1).
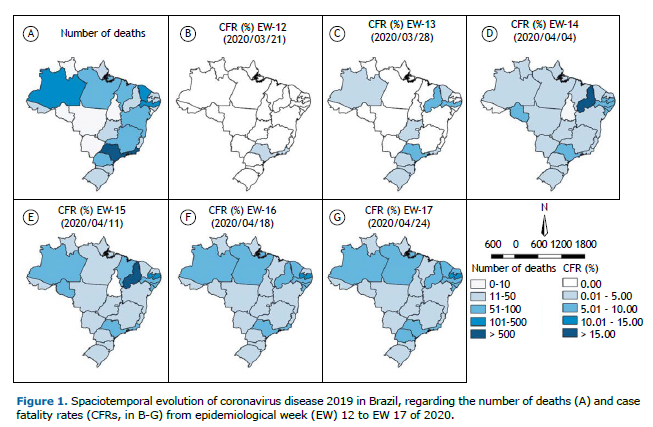
In EW 13, ten states accounted for 110 deaths: Santa Catarina, Rio Grande do Sul, Paraná, Rio de Janeiro, São Paulo, Goiás, Amazonas, Ceará, Pernambuco, and Piauí. The highest CFRs were found the states of Piauí (9.09%), Pernambuco (7.35%), and São Paulo (5.97%). In EW 14, there was an increase of 318 deaths and the number of accumulated deaths was 432, which was 3.8 times higher than in the previous week. Only the state of Tocantins reported no deaths. As can be seen in Figure 1, the highest CFRs were found in the states of Piauí (18.18%), Rondônia (9.09%), and Alagoas (8.70%).
In the following week (EW 15), 692 COVID-19-related deaths were added, bringing the national total to 1,124 (2.6 times higher than in EW 14). Of the ten states with the highest CFRs during that EW, six were in the northeastern region: Piauí (17.07%), Paraíba (12.94%), Sergipe (9.52%), Pernambuco (8.82%), Alagoas (6,25%), and Maranhão (6.10%). In EW 16, the cumulative number of deaths reached 2,346 (an increase of 1,222 in relation to the previous week), and COVID-19-related deaths had been reported in every state. The highest CFRs were observed in the states of Paraíba (12.68%), Pernambuco (9.35%), and Rio de Janeiro (8.52%). It is noteworthy that the state of Amazonas, which ranked 10th in CFR during EW 15 (5.05%), came to be ranked 4th by EW 16 (8.49%), as shown in Figure 1.
In EW 17, there were an additional 1,326 COVID-19-related deaths, bringing the total to 3,670. The numbers of confirmed deaths were highest in the states of São Paulo (n = 1,512), Rio de Janeiro (n = 570), and Pernambuco (n = 352), whereas the CFRs were highest in the states of Paraíba (11.40%), Rio de Janeiro (9.09%), and Pernambuco (8.80%), as can be seen in Figure 1.
Collectively, the states of São Paulo and Rio de Janeiro have a population of 63 million, which represents 29.7% of the population of Brazil. Although the first confirmed cases of COVID-19 and deaths from the disease were reported in those two states, it remains unclear whether they were the gateways for the disease to enter the country.(4)
It is of note that COVID-19-related mortality is determined not only by intrinsic characteristics of the infected individuals (age, previous diseases, and lifestyle) (5) but also by the access to and availability of therapeutic resources (hospital beds, health care staff, mechanical ventilators, and medications).(6) Therefore, the analysis of the lethality of the disease should take this combination of factors into account.
One study conducted in Brazil showed that the number of hospitalizations due to SARS between the confirmation of the first case of COVID-19 and EW 12 was higher than that found during the same period in previous years. The historical median of hospitalizations due to SARS in that EW is 299; in 2020, that number surpassed 1,000.(7)
By EW 13, all states in the southern region had reported COVID-19-related deaths. Those states (Rio Grande do Sul, Santa Catarina, and Paraná) have three important determinants of mortality(8): their populations are older than are those of other regions of the country(9); their historical incidence of SARS is the highest in the country(7); and they have a fragile health care network, albeit more structured than those in other regions of the country.(6) In addition, their proximity to the states of São Paulo and Rio de Janeiro represents an additional complicating factor, because it facilitates travel between the two regions.
In the northern and northeastern regions, social vulnerability is a chronic problem. This might explain why the states in those regions ranked highest regarding CFRs. Currently, Brazil has 32,757 ICU beds for adults, of which 14,873 (45.4%) are managed by the Brazilian Unified Health Care System. Of those ICU beds, only 227 (0.69%) and 454 (1.38%) are in the states of Piauí and Paraíba (6.9 beds/100,000 population and 11.2 beds/100,000 population, respectively), which had the highest CFRs between EW 13 and EW 17. In the northern region, the situation is more critical: the state of Amazonas, one of the epicenters of the pandemic in Brazil, has only 271 ICU beds (6.5 beds/100,000 population).(8)
It should be borne in mind that the CFR is influenced by the underreporting of confirmed cases and deaths. States where there is little testing or where testing is targeted only at critically ill patients tend to generate higher CFRs, because the actual number of patients is not reflected. In addition, there have been a great number of deaths for which the cause has not been identified or confirmed, which also affects the quality of the records.(10) Recent investigations have suggested that the number of infected individuals in Brazil might be 10 to 15 times greater than the number of reported cases.(10) Not knowing the true magnitude of the pandemic is an obstacle to fighting the disease.
The present study showed that spatiotemporal differences in the CFR of COVID-19 among Brazilian states might reflect social, economic, cultural, and structural inequalities. Therefore, there is no single solution for the whole country and health care policies must take regional particularities into consideration.
REFERENCES1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727-733. https://doi.org/10.1056/NEJMoa2001017
2. World Health Organization [homepage on the Internet] Geneva: World Health Organization; c2020 [updated 2020 Mar 11, cited 2020 Apr 26]. Coronavirus disease 2019 (COVID-19): Situation Report - 51. [Adobe Acrobat document, 9p.]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10
3. Johns Hopkins University [homepage on the Internet]. Baltimore (MD): the University; c2020 [cited 2020 Apr 26]. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE). Available from: https://coronavirus.jhu.edu/map.html
4. Brasil. Ministério da Saúde. Centro de Operações de Emergência em Saúde Pública [homepage on the Internet]. Brasília: o Ministério; c2020 [updated 2020 Apr 20; cited 2020 Apr 26]. Boletim COE COVID-19 no. 13: Situação epidemiológica--Doença pelo coronavírus 2019. [Adobe Acrobat document, 18p.]. Available from: https://portalarquivos.saude.gov.br/images/pdf/2020/April/21/BE13---Boletim-do-COE.pdf
5. Feng Y, Ling Y, Bai T, Xie Y, Huang J, Li J, et al. COVID-19 with Different Severity: A Multi-center Study of Clinical Features. Am J Respir Crit Care Med. 2020 Apr 10 [Epub ahead of print]. https://doi.org/10.1164/rccm.202002-0445OC
6. Fundação Oswaldo Cruz (FIOCRUZ) [homepage da internet]. Rio de Janeiro: FIOCRUZ; c2020 [updated: 2020 Mar 19; cited 2020 Apr 26]. COVID-19: relatório apresenta estimativa de infecção pelo vírus no país e os impactos no SUS [about 3 screens]. Available from: https://portal.fiocruz.br/noticia/covid-19-relatorio-apresenta-estimativa-de-infeccao-pelo-virus-no-pais-e-os-impactos-no-sus
7. Bastos LS, Niquini RP, Lana RM, Villela DAM, Cruz OG, Coelho FC, et al. COVID-19 and hospitalizations for SARI in Brazil: a comparison up to the 12th epidemiological week of 2020. Cad Saude Publica. 2020;36(4):e00070120. https://doi.org/10.1590/0102-311x00070120
8. Rache B, Rocha R, Nunes L, Spinola P, Malik AM, Massuda A. Necessidades de Infraestrutura do SUS em Preparo à COVID-19: Leitos de UTI, Respiradores e Ocupação Hospitalar (Nota Técnica n. 3). Instituto de Estudos para Políticas de Saúde, 2020 Mar.
9. Miranda GM, Mendes AC, Silva AL. Population aging in Brazil: current and future social challenges and consequences. Rev Bras Geriatr Gerontol. 2016;19(3):507-519. https://doi.org/10.1590/1809-98232016019.150140
10. COVID-19 Brasil [homepage on the Internet]. Ribeirão Preto: COVID-19 Brasil [cited 2020 Apr 28]. Monitoramento e análises da situação do Coronavírus no Brasil. Availa-ble from: https://ciis.fmrp.usp.br/













 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket