|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
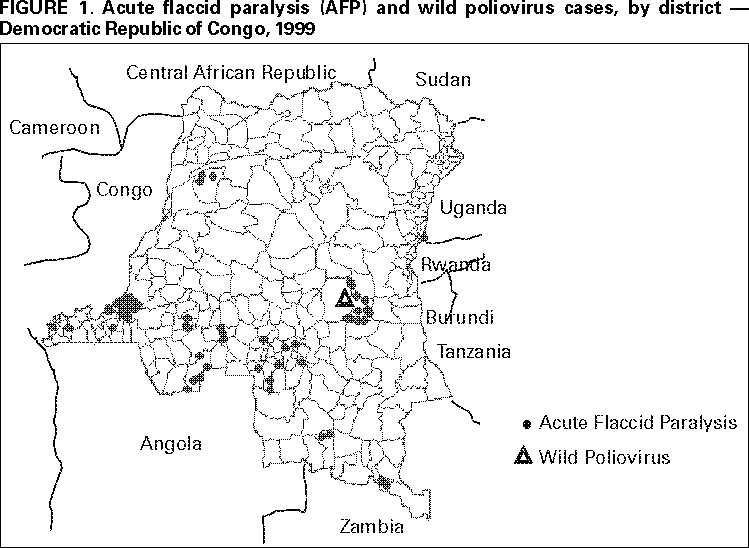
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- Democratic Republic of Congo, 1996--1999In 1988, the World Health Assembly resolved to eradicate poliomyelitis by December 31, 2000 (1). Although progress has been extraordinary (2), full implementation of polio eradication strategies has been delayed in several countries affected by war. The Democratic Republic of Congo (DRC) has experienced continual armed conflict since October 1996. As a result, DRC is the last country in the African Region of the World Health Organization (WHO) to implement National Immunization Days (NIDs*). DRC is an important global reservoir for wild poliovirus and shares more than 5580 miles (9000 km) of border with nine countries†; in at least seven of these countries polio is endemic. The large area of DRC, substantial amount of poverty, weak health-care infrastructure, poor transportation and communication, and competing demands for resources present considerable challenges to polio eradication. This report summarizes information on the existing health-care infrastructure and routine coverage, information from NIDs carried out in 1999, and results from the recently established surveillance system for acute flaccid paralysis (AFP). Existing Health-Care Infrastructure and Routine Vaccination CoverageDRC has an estimated population of 48.7 million persons§; 70% live in rural areas. As a result of armed conflict, health-care administration and logistics have become divided into two operational sectors. The western sector receives vaccine, cold chain equipment, and other supplies through Kinshasa while the eastern sector is supplied through Goma. The Ministry of Health (MOH) is supported by WHO, the United Nations Children's Fund (UNICEF), and national and international nongovernment organizations. In DRC during 1984--1995, mortality in infants (127 per 1000) and children aged <5 years (205 per 1000) remained static. Life expectancy is 45 years, and the maternal mortality rate is among the highest in the world (870 per 100,000 births). Expanded Program on Immunization (EPI) activities are coordinated by 42 subprovincial offices; each is headed by an EPI office and comprises several of the 307 health zones. Coverage in the western sector with three doses of oral poliovirus vaccine (OPV3) among children aged <1 year was an estimated 20%. Coverage with OPV3 in the eastern sector of North Kivu was 36% for the first 6 months of 1999. No data are available for the other eastern sector provinces where coverage is estimated to be lower. In 1998, a survey estimated 59% OPV3 coverage nationwide among children aged 12--23 months. Except for Angola (3), DRC is the only other African country where large outbreaks have been reported since polio eradication activities began in Africa in 1996. In 1995, approximately 1000 polio cases were reported in Mbuji May (Kasai Oriental). In 1997, 30 cases (and three deaths) were reported in Walikale (North Kivu), and 25 cases (no deaths) were reported in Inongo (Bandundu). In 1998, 87 cases (14 deaths) were reported in Walikale and seven cases (three deaths) in Kiri (Bandundu). National Immunization DaysDuring January--October 1996, Local Immunization Days (LIDs) were conducted in DRC's 32 most populous cities; 1,134,416 children aged 0-59 months (89% of the target population) received two doses of OPV. In 1997, LIDs were carried out in the 47 most populous cities and in 98 health zones along the eastern border. Reported coverage was 97% for Kinshasa and 80%--85% for other cities. In August 1998, the first NIDs were disrupted by the resumption of war. Although hostilities made nationwide implementation impossible, subnational NIDs were conducted in five of the country's 11 provinces; 3.4 million children (92% of the target population) were vaccinated with OPV. In 1999, three rounds of NIDs were planned for August, September, and October. The United Nations General Secretary arranged a cease-fire between the DRC government and the main opposing forces, and urged all factions to observe days of tranquility during NIDs. Vitamin A supplementation (4) was added to the second round of NIDs and measles vaccination to the third round in selected health zones. Because war created difficulty of movement between the eastern and western sectors, a team based in Goma planned and supervised NIDs for the eastern sector while the Kinshasa-based team planned and monitored NIDs for the western sector. Supplies for the east and west came through Goma and Kinshasa, respectively. Of the country's 307 health zones, 298 (97%) developed a plan to implement NIDs, and these plans were integrated into the overall national plan. Despite the agreement, on August 13, the first NIDs round, targeting all children aged 0--59 months, was disrupted by renewed fighting in the eastern sector; however, 80,000 health-care workers vaccinated in 11 provinces and 298 (97%) health zones were reached (Table 1). In nine health zones, no vaccination activity occurred; only one round was conducted in three zones (1%); 47 (15%) health zones conducted only two rounds. This accounts for the disparities in the numbers of children vaccinated in each round in some provinces (Table 1); 71%, 86%, and 81% of children in the target age group received OPV in the first, second, and third round, respectively; 6,098,500 (67%) children aged 6--59 months received a supplemental dose of vitamin A during the second round, and 3,321,832 children aged 9--59 months (80% of those targeted) were vaccinated against measles. AFP SurveillanceIn early 1999, AFP surveillance was initiated throughout DRC. The chief medical officers of each health zone are responsible for AFP surveillance and are supported by provincial EPI coordinators who report to the national EPI coordinator. Seven WHO sub-offices created in 1995 provide MOH with logistic and technical assistance for AFP surveillance activities. Although medical personnel have been trained in AFP surveillance in all provinces, surveillance is largely passive (there is no zero-case reporting from health facilities). From each of the 11 provinces, one national surveillance officer is recruited and provided with transportation. The National Institute for Biomedical Research was identified as the national polio reference laboratory and obtained WHO accreditation in December 1999. During 1999, 85 AFP cases were reported (Figure 1). All 85 had at least one stool specimen collected. Adequate¶ stool specimens were collected from 44 case-patients; 43 were negative for wild poliovirus and were classified as nonpolio. In 1999, three rounds of NIDs were planned for August, September, and October. Wild poliovirus type 3 was isolated from a stool specimen taken 30 days after onset of paralysis from a case-patient in Mbuji May (Kasai Oriental). Sixty-day follow-up examinations were not conducted for the 41 cases with inadequate specimens, which were confirmed as polio on clinical case classification criteria**. The overall nonpolio AFP rate was 0.17 per 100,000 children aged <15 years. Reported by: World Health Organization (WHO) Country Office, Kinshasa, Democratic Republic of Congo (DRC); United Nations Children's Fund (UNICEF) Country Program, Kinshasa, DRC. Regional Office for Africa, WHO, Harare, Zimbabwe. Regional UNICEF Office for West and Central Africa Region, Abidjan, Côte d'Ivoire. UNICEF, New York. Vaccines and Biologicals Dept, WHO, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Vaccine Preventable Disease Eradication Div, National Immunization Program, CDC. Editorial Note:The goal of global polio eradication will not be achieved unless strategies are implemented effectively in all countries where polio is endemic, including those affected by civil unrest or war. This report from DRC, together with reports from Afghanistan (5), Somalia, southern Sudan (6), and other war-torn areas (7), suggests that even under extremely adverse conditions, effective polio eradication strategies can be implemented. NIDs in DRC that reached almost all health zones and the initiation of AFP surveillance demonstrate that armed conflict does not present an insurmountable barrier to implementing eradication strategies. Despite the successes, however, future NIDs must cover all areas of the country. Nine health zones, with a combined target population of 270,000 children aged <5 years, were not reached during the 1999 NIDs; conflict prevented another 57 health zones from completing OPV3 rounds. In 2000, a cease-fire, days of tranquility for NIDs respected by all armed groups, and completion of three NIDs rounds in all 307 DRC health zones are factors critical to eradication efforts. Plans for polio eradication in DRC in 2000 include strengthening routine EPI; conducting three rounds of intensified NIDs in July, August, and September 2000 (including house-to-house vaccination in much of the country); and expanding AFP surveillance. The long-term success of NIDs in DRC requires the negotiation of a formal cease-fire; the strong commitment of the DRC government; a solid partnership between MOH, United Nations agencies, and other organizations; commitment of the necessary funds and resources to overcome the limitations of the existing infrastructure; and a decentralized approach to planning and implementation. The detection of 85 AFP cases also demonstrates that AFP surveillance can be initiated in countries affected by war and limited infrastructure. Cases already have been reported from nine of the country's 11 provinces. The success is primarily the result of MOH commitment and the establishment of a surveillance infrastructure. The sensitivity, quality, and geographic extent of AFP surveillance must be enhanced to ensure that data can be used to target mopping-up activities as polio transmission becomes focused in DRC. Active surveillance with zero-case reporting from the main referral hospitals must be initiated. If DRC is to eradicate polio by the end of 2000, the necessary human, material, and financial resources must be made available in a timely manner††. International, national, and local efforts pressing for peace or at least access to children for vaccination and other health activities must be a priority. References
* Nationwide mass campaigns over a short period (days to weeks), in which two doses of oral poliovirus vaccine are administered to all children in the target age group (usually aged <5 years), regardless of vaccination history, with an interval of 4--6 weeks between doses. † Angola, Burundi, Central African Republic, Congo, Rwanda, Sudan, Tanzania, Uganda, and Zambia. § Based on the results of the 1999 NIDs. ¶ Two stool specimens collected at an interval of at least 24 hours within 14 days of paralysis onset. ** AFP cases are confirmed as polio if wild poliovirus is isolated from two specimens, if follow-up examinations 60 days after onset show residual paralysis, or if no follow-up could be conducted (i.e., patient died or was lost to follow-up). †† Polio eradication in DRC is supported by the DRC government; external support is provided by WHO, UNICEF, Rotary International, and the government of the United States (through U.S. Agency for International Development and CDC).
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 3/30/2000 |
|||||||||
This page last reviewed 5/2/01
|