 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- West and Central Africa, 1999--2000In 1988, the World Health Assembly of the World Health Organization (WHO) resolved to eradicate poliomyelitis by 2000 (1). Reported polio cases have decreased on all continents. In 2000, poliovirus was isolated from 24 countries, 13 in the African Region of WHO (AFR). This report summarizes the routine polio vaccination coverage, surveillance for acute flaccid paralysis (AFP*) during 1999 and 2000, and the synchronization of national immunization days (NIDs†) against polio during 2000 and early 2001 in 16 countries in west and central Africa§. Routine VaccinationDuring 1999, routine vaccination coverage with three doses of oral poliovirus vaccine (OPV3) among infants aged 1 year was approximately 48% in the 16 countries (range: 12%--90%) (Table 1). In comparison, reported OPV3 coverage in AFR was approximately 55% in 1999 and has remained relatively stable since 1990 (2). AFP SurveillanceDuring 2000, AFP surveillance improved in all countries except Chad and Côte d' Ivoire (Table 1). The number of confirmed polio cases in the West Africa Region, Cameroon, and Chad decreased from 1309 in 1999 to 879 in 2000. The number of polio cases confirmed by wild virus isolation decreased from 186 in 1999 to 41 in 2000 (Table 1). With the exception of Ghana, Côte d'Ivoire, and Niger, the proportion of AFP cases with adequate specimens substantially increased in all countries from 26%--74% in 1999 to 37%--84% in 2000. Synchronization of NIDsMost of the countries in west and central Africa have conducted annual NIDs since 1996. Despite the progress achieved by these countries, wild poliovirus was still circulating during 2000. To maximize the number of susceptible children reached during NIDs, 14 contiguous countries in the West Africa Region and Cameroon and Chad conducted synchronized NIDs against polio during October and November 2000 and January 2001. The WHO intercountry program (ICP) office in Abidjan, Côte d'Ivoire, coordinated this effort¶. Coordinated cross-border activities were implemented by 14 of the 16 countries. Planning meetings for these activities were conducted in four border towns corresponding to the following country cross-border activities: 1) Senegal-Gambia-Guinea--Bissau; 2) Côte d'Ivoire-Mali-Burkina Faso; 3) Burkina Faso-Ghana-Togo; and 4) Benin-Niger-Nigeria (Figure 1). Inclusion of high-risk and special populations living in border areas were considered, and special resources were allocated to the border districts for the implementation of this activity. Approximately 300,000 health personnel were trained and mobilized for implementation of the synchronized NIDs, and approximately 180 million doses of OPV were distributed to participating countries. The estimated number of children vaccinated increased from 65 million in 1999 to 77 million in November 2000 (Table 2). In all countries except Senegal, the proportion of children vaccinated in 2000 was greater than that during the 1999 NIDs. In addition, the number of children aged <5 years vaccinated for the first time decreased from 1,326,476 in October 2000 to 1,161,283 in November 2000. Reported by: World Health Organization Inter-Country Program Office, Abidjan, Côte d'Ivoire. Expanded Program on Immunization, World Health Organization, Regional Office for Africa, Harare, Zimbabwe. Vaccines and Biologicals Dept, World Health Organization, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Vaccine Preventable Disease Eradication Div, National Immunization Program, CDC. Editorial Note:Substantial progress in polio eradication occurred during 1999--2000 in west and central Africa. Poliovirus transmission can be interrupted in the remaining countries where polio is endemic if vaccination activities are of high quality and NIDs continue to be synchronized within major epidemiologic blocs. The synchronization of NIDs in west and central Africa during 2000 and early 2001 is expected to reduce and eventually eliminate wild poliovirus transmission. NIDs have resulted in millions of children being vaccinated against polio who otherwise would not have been reached. The strategies used during NIDs have included fixed-posts**, house-to-house††, and a combination of the two approaches. High-quality house-to-house vaccination campaigns are essential for reaching susceptible children in high-risk areas, including border areas with large population movements. Coordinated multicountry vaccination campaigns have been conducted previously. Since 1995, synchronized mass campaigns conducted by 18 countries from the Middle East, Central Asia, and the Caucasus regions (MECACAR) achieved high vaccination coverage. Approximately 62 million children, 95% of children aged <5 years, were vaccinated every year during 1995--1997 (3,4). A high level of political support in the 16 countries enabled implementation of NIDs. Heads of state and other prominent political leaders were involved in all stages of the activity. Three of the participating countries experienced civil unrest or war at the time of the NIDs. However, all three implemented NIDs and conducted cross-border activities, demonstrating that polio eradication activities can be implemented in countries in conflict and can promote peace building. Rival factions agreed to respect cease-fires so that children could be vaccinated. Additional potential peace-building efforts were demonstrated by the interaction between the ministries of health, external affairs, and other bodies of the government with their counterparts from neighboring countries fostered by the cross-border activities. The advantages of such collaborations are that other public health programs could benefit from the networks developed for the synchronized NIDs. The synchronized polio campaign in Africa resulted in improvements in the infrastructure of national vaccination programs through strengthening of the Expanded Program on Immunization in specific areas, such as cold chain and vaccine distribution systems, and through additional training of health professionals. Experiences during this campaign will be useful in planning and implementing synchronized NIDs in central Africa, which are scheduled for later this year. The lack of experience implementing the house-to-house strategy and poor micro- planning in some countries were limitations in implementing synchronized NIDs in west and central Africa. Additional efforts will be required to coordinate efficiently the flow of information and data management at the ICP office in Abidjan. These problems may be addressed by 1) earlier planning of NIDs; 2) centralizing the information at the ICP coordinating office; 3) improving mapping and microplanning at the smallest administrative unit; 4) maintaining more efficient field supervision of vaccination teams; and 5) allocating sufficient staff to identify more quickly and correct problems. A decrease in the number of polio cases this year will be the best indicator of the quality of the synchronized campaign in west and central Africa. The success in the implementation of synchronized NIDs should encourage other epidemiologic blocs to use the same strategy. Certification of global polio eradication by 2005 will require continued synchronized mass vaccination campaigns and high-quality AFP surveillance. References
*AFP surveillance is a monitor of the sensitivity of detection and accuracy of reporting suspected cases (target: an annual rate of >1 nonpolio AFP cases per 100,000 children aged <15 years). † Nationwide mass campaigns over a short period (days to weeks), in which two doses of oral poliovirus vaccine are administered to all children in the target group (usually aged <5 years), regardless of vaccination history, with an interval of 4--6 weeks between doses. § Benin, Burkina Faso, Cameroon, Chad, Gambia, Ghana, Guinea, Guinea-Bissau, Côte d' Ivoire, Liberia, Mali, Niger, Nigeria, Senegal, Sierra Leone, and Togo. Initially, Mauritania also was included; however, logistic problems prohibited Mauritania from participating in the synchronized NIDs. ¶ The polio eradication initiative in AFR is supported by member countries. External funding is provided by Rotary International; United Nations Children's Fund; the governments of Canada, United States, United Kingdom, Norway, and Belgium; the United Nations Foundation; the Gates Foundation; the De Beers Corporation; WHO; and CDC. ** Parents bring their children to a specific health post for vaccination on a predetermined date(s). †† Health-care workers vaccinate children by going from one house to the next on a predetermined date(s). Table 1  Return to top. Figure 1  Return to top. Table 2 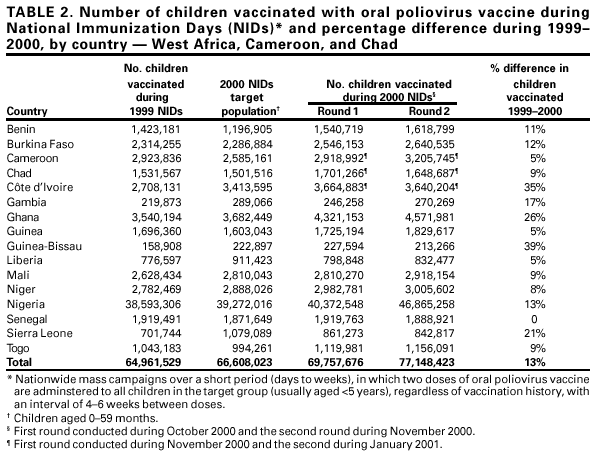 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/15/2001 |
|||||||||
This page last reviewed 6/15/2001
|