|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
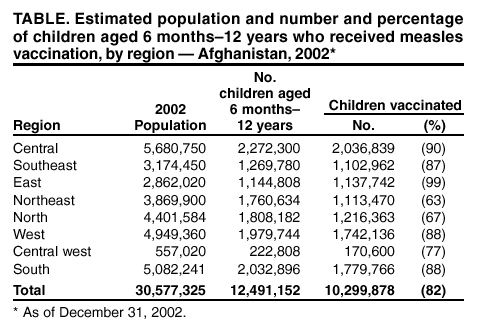
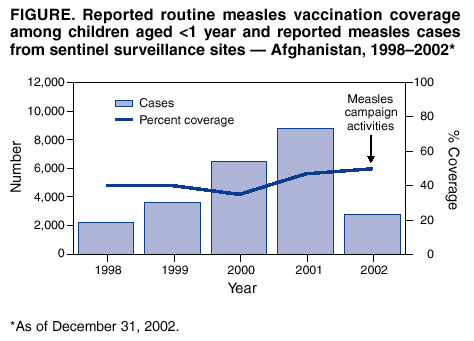
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Nationwide Measles Vaccination Campaign for Children Aged 6 Months--12 Years --- Afghanistan, 2002The public health infrastructure in Afghanistan has been devastated by 23 years of civil war, and both the infant mortality rate (165 per 1,000 live-born infants) and the mortality rate for children aged <5 years (256 per 1,000 live-born infants) are among the highest in the world (1,2). The major causes of death among children aged <10 years are diarrhea (32%), measles (25%), respiratory tract infections (13%), and other causes (30%), including malnutrition, scurvy, chronic diseases, and fever of unknown origin (3). Measles accounts for an estimated 30,000--35,000 deaths each year in Afghanistan (4). To reduce measles-related mortality, during 2002, the Ministry of Health (MoH) of the Interim Government of Afghanistan, with the support of international organizations, organized a nationwide measles vaccination campaign for children aged 6 months--12 years. This report describes the planning, implementation, and impact of this campaign. The findings suggest that the campaign had a major impact on reducing measles-related mortality. Similar campaigns might be feasible in countries affected by complex emergencies. Before implementation of the campaign, routine measles vaccination coverage was low. During 1998--2001, reported coverage with 1 dose of measles vaccine among infants in Afghanistan was 40%--47% (MoH/United Nations Children's Fund [UNICEF] country office, Afghanistan, unpublished data, 2002) (Figure). During 2001, among infants in Afghanistan, reported coverage was 45% for 3 doses of combined diphtheria-tetanus-pertussis (DTP) vaccine, 46% for 3 doses of oral poliovirus vaccine (OPV), and 47% for measles vaccine (5). Polio National Immunization Days (NIDs)* served as a model for the measles vaccination campaign. Polio NIDs have been conducted throughout Afghanistan since April 1997 and subnational immunization days (SNIDs)† in some provinces since 1994 (6). Reported coverage achieved by NIDs has increased from 80% in 1997 to 99% in 2002 (MoH/UNICEF country office, Afghanistan, unpublished data, 2002). Because of the success of NIDs in reaching children, confirmed polio cases declined from 150 in 1999 to 11 in 2001 and 10 in 2002 (7,8). Measles sentinel surveillance data were used to determine the target age group for the nationwide measles vaccination campaign. During 2001, a total of 8,762 cases of measles were reported through the country's 356 sentinel surveillance sites (9) (Figure). Of these 8,762 persons with measles, 8,356 (95%) were children aged <12 years (age distribution: aged <1 year, 8%; aged 1--5 years, 57%; aged 5--12 years, 35%) (World Health Organization [WHO], Afghanistan, unpublished data, 2001). This age group was targeted because measles vaccination campaigns in Africa have indicated that targeting only children aged 9 months--5 years might allow transmission to continue among children aged >5 years, who then spread the measles virus to susceptible younger siblings, resulting in ongoing mortality from measles (10). In late 2001, an influx of approximately 2 million refugees returning from Pakistan and other neighboring countries was anticipated in Afghanistan in 2002. Acute and chronic malnutrition were prevalent and outbreaks of measles resulting in thousands of deaths were anticipated. In response, MoH, UNICEF, and WHO targeted children aged 6 months--12 years for measles vaccination and raised $8 million§ to support the campaign. Because the large influx of returning refugees increased uncertainty about the size of the target population, data from the most recent polio NIDs (2001--2002) were used to estimate the population aged 6 months--12 years. The number of children aged <5 years vaccinated during NIDs was used to estimate the denominator of children aged 5--12 years by assuming equal annual birth cohort sizes among children of both age groups. To reinforce safe vaccine handling, injection technique, and waste management, training sessions were organized for 30 trainers who were responsible for training vaccination teams. Each trainer was responsible for training approximately 500 vaccinators (estimated total: >15,000 vaccinators). To ensure the safety and quality of the campaign, vaccination teams were instructed to vaccinate <200 children per day in urban areas and <70 in rural areas. Auto-disable syringes and safety boxes were used at all vaccination sites. The nationwide measles vaccination campaign was conducted throughout 2002, initially targeting high-risk districts and cities with the largest number of susceptible children, and subsequently the most remote and inaccessible villages. Vaccination sites were established in local mosques with the support of the community and religious leaders. Incoming refugees were vaccinated on entry at registration points along the borders with Iran and Pakistan. Approximately 40 international agencies and nongovernment organizations assisted with the transport of teams and supplies to an estimated 1,200 fixed vaccination sites (e.g., markets, mosques, and health centers) and 3,000 mobile clinics. In October 2002, a review was performed in each district to determine measles vaccination coverage by using a range of denominators, including projected populations from the 1979 census and the 2002 polio NIDs. All children in districts with a mean coverage of <80% (using projections from 2002 NIDs) during the campaign were revaccinated, regardless of previous vaccination. As of December 31, 2002, a total of 10,299,878 children were reported to have been vaccinated, representing 82% of the national target population (Table). During 2001--2002, the number of reported measles cases decreased from 8,762 to 2,574. The cost of the campaign was approximately $0.78 per child vaccinated (external donor costs only). No deaths associated with measles vaccination were reported during the campaign. However, because a monitoring system for adverse events had not yet been established, some adverse events might have been missed. In one village, a cluster of 150 children with abscesses at the vaccine injection site attributable to poor vaccination technique was reported (MoH/UNICEF country office, Afghanistan, unpublished data, 2002). Reported by: F Feroz, A Sherzai, A Ashgar, Expanded Program of Immunization, Interim Government Ministry of Health; P Salama, T Naleo, A Ansari, N Dadgar, A Golaz, United Nations Children's Fund Country Office; N Sadozai, H Eskander, I Reza, H Jafari, World Health Organization, Afghanistan Country Office, Kabul, Afghanistan. E Hoekstra, A Paganini, Y Bergevin, United Nations Children's Fund Headquarters, New York, New York. M Brennan, Div of Emergency Environmental Health Svcs, National Center for Environmental Health; F Lievano, Global Immunization Div, National Immunization Program, CDC. Editorial Note:This is the first nationwide measles vaccination campaign for a broad age range (children aged 6 months--12 years) implemented in a country affected by a complex emergency. The marked reduction of reported measles cases and the estimated high vaccination coverage indicate that the campaign probably had a major impact on reducing measles-related mortality. Similar campaigns might be feasible in other countries affected by complex emergencies if adequate resources are provided and careful planning and appropriate training are conducted. A better understanding of the campaign's impact in reducing measles cases and deaths is expected when measles incidence data for 2003 become available. Rapid identification and training of vaccination teams for the measles campaign in Afghanistan was made feasible by the existing network of vaccinators trained through the polio eradication program. Training sessions for additional vaccinators were conducted (1 week per team), and detailed plans were drafted at the provincial and district level to implement the campaign. In addition, the measles campaign supported the November 2002 polio NIDs by identifying children who had not been vaccinated previously against polio. The measles campaign faced many challenges, including 1) inadequate security in some areas; 2) difficulty in accessing several regions in the country, particularly during the winter; and 3) the lack of an adverse events surveillance system. Previous experiences gained during NIDs, including detailed mapping of population settlements, helped to identify communities with the largest target populations. Additional benefits of the campaign that might strengthen the routine vaccination program include the improvement of the cold chain and increased social awareness about disease prevention through vaccination. Finally, the social mobilization necessary for the success of this public health initiative throughout markets and mosques in every district of the country might contribute to other public health efforts in Afghanistan. Future plans to strengthen measles control in Afghanistan include improved surveillance for vaccine-preventable diseases and strengthening the routine measles vaccination program by applying strategies used in this campaign (e.g., mosque-to-mosque vaccination) to improve routine coverage in remote areas. References
§ In addition to the United Nations Foundation, donor countries for the measles campaign in Afghanistan were Australia, Canada, Finland, Germany, Italy, Japan, Poland, the United Kingdom, and the United States. * Mass campaigns over a short period (days to weeks) in which 2 doses of OPV is administered to all children in the target group (usually aged 0--4 years) regardless of previous vaccination history, with an interval of 4--6 weeks between doses. † Campaigns similar to NIDs but confined to part of the country.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 4/24/2003 |
|||||||||
This page last reviewed 4/24/2003
|