|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
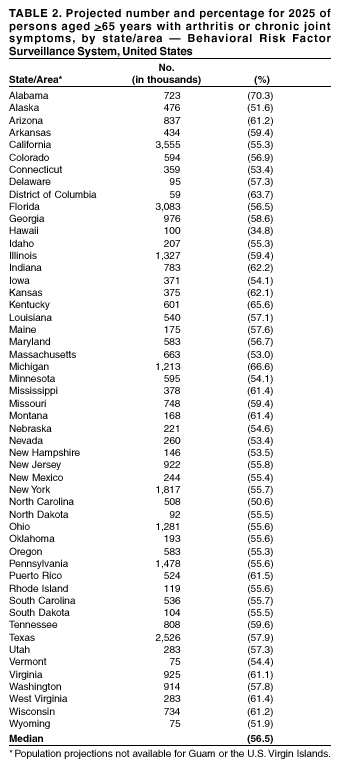
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Public Health and Aging: Projected Prevalence of Self-Reported Arthritis or Chronic Joint Symptoms Among Persons Aged >65 Years --- United States, 2005--2030Arthritis and other rheumatic conditions are among the most common chronic diseases, affecting 70 million U.S. adults in 2001 (1), and comprise the leading cause of disability among U.S. adults (2). Arthritis prevalence increases with age, affecting approximately 60% of the U.S. population aged >65 years (1). As a result of better identification and treatment of other chronic diseases and lower mortality from infectious diseases, U.S. adults are living longer, and the U.S. population is aging (3). For this reason, the number of persons living with nonfatal but disabling conditions such as arthritis or chronic joint symptoms (CJS) might be increasing. To estimate the projected future burden of arthritis or CJS among persons aged >65 years, CDC applied data from the 2001 Behavioral Risk Factor Surveillance System (BRFSS) to projected national population data for 2005--2030 and state population data for 2025. This report summarizes the results of that analysis, which indicate that if arthritis prevalence rates remain stable, the number of affected persons aged >65 years will nearly double by 2030. Proven public health interventions should be applied and new interventions developed to improve function, decrease pain, and delay disability among persons with arthritis, particularly those at highest risk for functional impairment and disability. BRFSS is a state-based, random-digit--dialed telephone survey of the U.S. civilian, noninstitutionalized population aged >18 years. BRFSS is administered in all 50 states, the District of Columbia, and three U.S. territories (Guam, Puerto Rico, and the U.S. Virgin Islands) (4). The median response rate in 2001 was 51.1% (range: 33.4% [New Jersery]--81.5% [Puerto Rico]). Respondents were classified as having CJS if they answered "yes" to two questions: "In the past 12 months, have you had pain, aching, stiffness, or swelling in or around a joint?" and "Were these symptoms present on most days for at least a month?" Respondents were considered to have physician-diagnosed arthritis if they answered "yes" to the question, "Have you ever been told by a doctor that you have arthritis?" Respondents reporting either CJS or physician-diagnosed arthritis were classified as having arthritis or CJS. Respondents who did not know, were not sure, or refused to answer were classified as not having either condition. Sex-specific prevalence rates (males: 51.6%; females: 63.9%) for arthritis or CJS among persons aged >65 years were multiplied by the sex-stratified U.S. Census projections of the population aged >65 years (5) for a year and summed to produce national arthritis or CJS prevalence projections, which were reported in 5-year intervals for 2005--2030. State-specific prevalence projections also were calculated by applying 2001 BRFSS state prevalence rates to U.S. Census projections for 2025, the latest year for which state-specific projected population estimates were available. During 2005--2030, the percentage of the U.S. population aged >65 years is expected to increase from 12.9% to 20.0% (Table 1). If sex-specific prevalence rates remain the same for this population, the number of persons aged >65 years projected to have arthritis or CJS will nearly double, from 21.4 million in 2005 to 41.1 million in 2030. The percentage of persons aged >65 years projected to have arthritis or CJS in 2025 varied by area (median: 56.5%; range: 34.8% [Hawaii]--70.3% [Alabama]); in 11 states and Puerto Rico, approximately 60% of persons aged >65 years will have arthritis or CJS by 2025 (Table 2). Reported by: JM Hootman, PhD, CG Helmick, MD, G Langmaid, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that by 2030, approximately 41 million persons aged >65 years will have arthritis or CJS, with a median state-specific prevalence of 56.5% by 2025. Previous lower projections of arthritis cases by 2020 (6) were based on rates for persons of all ages and used a different case definition from the 1989--1991 National Health Interview Survey. The broader BRFSS case definition includes persons with arthritis or those with CJS indicative of arthritis whose condition might be undiagnosed. The findings in this report are subject to at least five limitations. First, projected prevalence estimates were based on rates calculated from self-reported data that were not confirmed by a physician. Second, BRFSS excludes military personnel residing on bases, institutionalized populations, and persons without telephones. Third, the median response rate in this survey (51.1%) was low; however, BRFSS demographics mirror U.S. Census distributions. Fourth, the 2001 BRFSS case definition might include some persons with acute, self-limiting musculoskeletal injuries rather than arthritis. To improve sensitivity, the 2002 BRFSS questions were changed; studies validating these questions are under way. Finally, the projected estimates presented in this report might be conservative because the analysis assumed steady age- and sex-specific rates of arthritis, and other factors affecting the prevalence of arthritis (e.g., therapy and the obesity epidemic) were not considered. To help the large numbers of older adults manage their arthritis or CJS, viable and affordable programs should be available at the community level (7). CDC's Arthritis Program funds 36 state health departments to enhance public health activities for arthritis. State programs disseminate evidence-based interventions, including the Arthritis Foundation's PACE® (People with Arthritis Can Exercise) and aquatics programs, and self-management education classes such as the Arthritis Self-Help Course. These interventions have reduced the impact of arthritis or CJS by improving function and reducing pain and the need for physician visits (8). Additional information about CDC-funded state arthritis programs and evidence-based interventions is available at http://www.cdc.gov/nccdphp/arthritis. The aging of the population is a critical issue facing the U.S. public health, medical, and economic systems (3,9). Arthritis contributes substantially to disability, poor health-related quality of life, and increased direct and indirect medical costs (3,10). Decreasing this impact will require effective public health interventions that improve function, decrease pain, and delay disability among persons with arthritis. Fewer than 1% of persons with arthritis who could benefit from such interventions receive them (10). Specific interventions targeted toward persons with arthritis who are at highest risk for functional impairment and disability (e.g., persons who are overweight/obese or physically inactive) also should be developed. References
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 5/29/2003 |
|||||||||
This page last reviewed 5/29/2003
|