|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
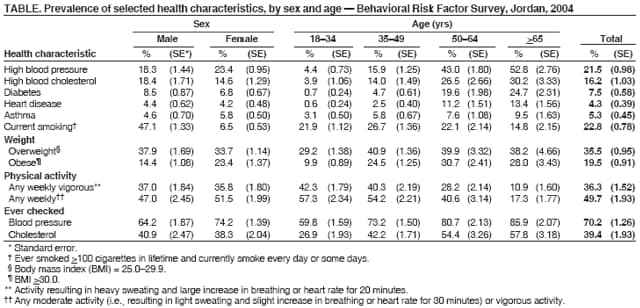
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Assessing Risk Factors for Chronic Disease --- Jordan, 2004In 2003, chronic diseases were the leading cause of mortality in Jordan; 38.2% of deaths were attributed to cardiovascular disease and 14.3% to cancer (Jordan Ministry of Health [MOH], unpublished data, 2004). In 2002, MOH, with assistance from CDC and the World Health Organization (WHO), established a behavioral risk factor surveillance program to monitor risk factors associated with chronic diseases (1). This report summarizes the findings of the second Behavioral Risk Factor Survey, which was conducted in Jordan in 2004. The findings indicated that the prevalence of obesity had increased by 52.3% in Jordan since 2002. In addition, cancer screening rates among women and seatbelt use rates overall were low compared with U.S. rates. Development and implementation of a national plan to prevent and control chronic diseases is needed. The first national Behavioral Risk Factor Survey in Jordan, conducted in 2002, was created by adding questions to the quarterly, multistage, cross-sectional employment survey from the Jordan Department of Statistics. The 2004 Behavioral Risk Factor survey was conducted by MOH using similar sampling methodology but included additional questions on chronic disease risk factors. The survey was conducted among a nationally representative sample of adults aged >18 years. In each household, one adult was selected randomly and interviewed in person. Interviews were conducted during October 1--December 13, 2004; a total of 3,334 adults were interviewed (response rate: 94.7%). The survey included questions on demographics, health status, health-care access, hypertension awareness, cholesterol awareness, diabetes, asthma, heart disease, tobacco use, seatbelt use, physical activity, nutrition, weight and height, oral health, eyesight, women's health, medical services, and screening. Data on self-reported weight and height were used to calculate body mass index (BMI) (kg/m2). Overweight was classified as a BMI of 25.0--29.9, and obese was classified as a BMI of >30.0. Weights and heights were self reported. For cultural reasons, only married women were asked how long it had been since their most recent Papanicolaou test; all women aged >35 years were asked how long it had been since their most recent mammogram. All respondents were asked whether they had ever had their blood pressure or cholesterol level checked by a health-care professional and whether a health-care professional had ever told them they had high blood pressure, high cholesterol, asthma, or diabetes. Screening for diabetes complications was assessed by asking, "How many times during the last 12 months has a health professional checked your feet for any sores or irritations?" and "When was the last time you had an eye exam by an ophthalmologist?" Gestational diabetes was excluded, and type of diabetes was not assessed. Health status was assessed by asking, "Would you say that in general your health is excellent, very good, good, fair, or poor?" Vigorous physical activity was assessed by asking, "On average, how many days a week do you get at least 20 minutes of vigorous physical activity?" Moderate physical activity was assessed by asking, "On an average, how many days a week do you get at least 30 minutes of moderate physical activity?" Seatbelt use was assessed by asking, "Do you always use a seatbelt when you drive a car?" and "Do you always use a seatbelt when sitting next to the driver?" Fruit and vegetable consumption was assessed by asking, "How many cups of fresh or cooked vegetables did you have yesterday?" and "How many cups of fruit or fresh juice did you have yesterday?" Statistical analysis software was used to account for the complex sampling design. The prevalence of obesity among Jordanian adults increased to 19.5% in 2004, a 52.3% increase from the 2002 prevalence of 12.8% (1) (Table). In 2004, approximately 55.0% of adult respondents (52.3% of men and 57.1% of women) were categorized as either overweight or obese, an increase from the 2002 prevalence of 45.2%. Weight awareness was inconsistent, with 27.8% of obese respondents reporting that they considered their weight to be nearly average; in 2002, 22.2% of obese respondents considered their weight to be average. Approximately 19.5% of the respondents reported consuming three or more cups of fruit, fresh juice, or vegetables the preceding day. The prevalence of diagnosed diabetes increased from 6.4% in 2002 to 7.5% in 2004, although this increase was not statistically significant. Approximately 24.7% of respondents aged >65 years had diagnosed diabetes. Among all respondents with diabetes, 62.9% reported they had not had their feet checked for sores or irritations, and 45.3% had not had an eye examination in the preceding 12 months. Among persons with diabetes who had ever had an eye examination, 36.3% were told they had eye complications. Approximately 5.3% of all respondents reported that they had been told they had asthma, a rate similar to that of the 2002 survey (5.1%). Approximately 13.3% of respondents reported their health as fair or poor, and 26.5% said it was good. Cancer screening rates among women were low compared with rates from the 2004 U.S. Behavioral Risk Factor Surveillance System survey (2). Approximately 14.9% of married women reported having had a Papanicolaou test in the preceding 3 years in Jordan, compared with 86.0% of women aged >18 years in the United States; 9.3% of women aged >40 years reported having had a mammogram in the preceding 2 years, compared with 74.9% of U.S. women aged >40 years. Approximately 70.2% of respondents had ever been tested for high blood pressure, and 39.4% had ever had their cholesterol levels checked. Because some questions in the 2004 Jordanian survey were changed, no direct comparisons between the 2002 and 2004 surveys could be made for blood pressure, cholesterol, or smoking status. Approximately 61.6% of drivers and 40.4% of front-seat passengers reported always using a seatbelt, compared with 80.5% of U.S. drivers in 2002 (3). Reported by: A Belbeisi, MD, M Zindah, MD, Jordan Ministry of Health. H Walke, MD, B Jarrar, AH Mokdad, PhD, Div of Epidemiology and Surveillance Capacity Development, Coordinating Office for Global Health, CDC. Editorial Note:Estimates of the extent of obesity and diabetes in Jordan are conservative. In validation studies of self-reported weight and height, overweight participants tend to underestimate their weight, and all participants tend to overestimate their height (4). Moreover, undiagnosed diabetes cases were excluded. On the basis of findings from the 2004 survey, the Jordanian cabinet allocated $2.9 million for chronic disease prevention and control. Higher-than-normal BMI and weight gain are major risk factors for diabetes (5), and other studies have indicated that changes in BMI at the population level foreshadow changes in diabetes prevalence (6,7). Obesity and diabetes usually are preventable. Previous studies have demonstrated that changes in lifestyle can prevent diabetes and obesity in selected groups of adults at high risk (8,9). The low rates of screening practices among residents of Jordan should be addressed. Screening and early diagnosis of chronic diseases are important for preventing related complications and death. For example, the high rate of eye complications among persons with diagnosed diabetes is an indication of a delay in diagnosis and proper management of the disease. Increasing awareness about chronic disease risk factors among health-care workers and the public is critical. Adequate and continuous monitoring of chronic disease risk factors in Jordan is needed, and the surveillance findings should be used in disease-prevention and health-promotion activities. The findings in this report are subject to at least four limitations. First, the survey is cross-sectional and was not conducted throughout the year; therefore, some of the behaviors that vary seasonally (e.g., dietary intake) might not be representative. Second, the design does not allow determination of causality. Third, all the variables were self reported, which might have resulted in self-report bias. Finally, only the prevalence of diagnosed diseases could be assessed; therefore, the reported prevalence of chronic diseases is an underestimation because only 55% of respondents reported having had a medical checkup in the preceding 6 months. The Jordan Field Epidemiology Training Program (FETP) and MOH are developing and implementing a national chronic disease prevention and control plan. This plan will target primary risk factors and behaviors associated with chronic diseases (e.g., smoking, overweight, unhealthy diet, and physical inactivity) and call for collaboration among all governmental ministries, nongovernmental organizations, and the private sector. Although many countries are improving their health infrastructure, chronic diseases continue to be a public health problem. In addition, the high cost of chronic disease treatment puts an additional strain on countries with developing economies (10). More global collaboration and partnerships in chronic disease prevention and control are needed; certain FETPs (e.g., in Egypt and China) have begun working to address the problem. Acknowledgment The findings in this report are based, in part, on contributions by the Jordan Field Epidemiology Training Program. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/15/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|