|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
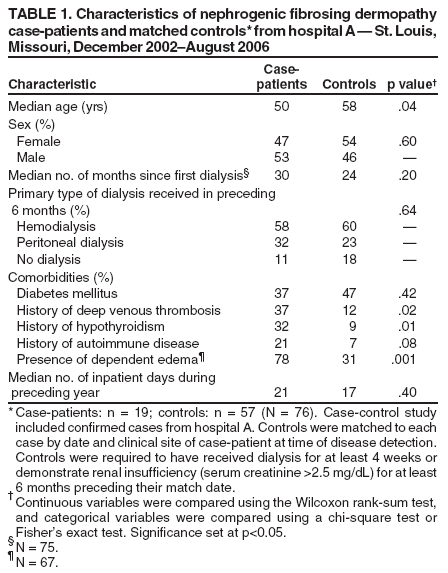
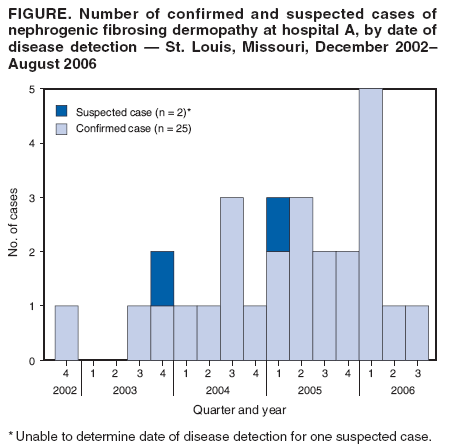
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Nephrogenic Fibrosing Dermopathy Associated with Exposure to Gadolinium-Containing Contrast Agents --- St. Louis, Missouri, 2002--2006Nephrogenic fibrosing dermopathy (NFD) causes thickening and hardening of the skin, often in the extremities, and occurs in patients with underlying renal disease. The skin lesions can progress rapidly, sometimes leading to joint immobility and the inability to walk (1). In May 2006, nephrologists at hospital A in St. Louis, Missouri, reported to CDC and the Missouri Department of Health and Senior Services (MoDHSS) a cluster of NFD among patients treated in their dialysis units. CDC and MoDHSS conducted an investigation to determine the number of affected patients and identify risk factors for NFD. Thirty-three patients with NFD were identified in St. Louis, 28 of whom had been treated at hospital A. A matched case-control study was conducted at the hospital. This report summarizes the preliminary results of that study, which indicated that exposure to gadolinium-containing contrast agents during magnetic resonance imaging (MRI) studies was independently associated with NFD. Clinicians should be aware of the potential for NFD, and when possible, should avoid use of gadolinium-containing contrast agents in patients with advanced renal disease. A confirmed case was defined as clinical findings (i.e., skin thickening or hardening) and skin biopsy findings consistent with NFD in a person with renal disease in St. Louis during January 2000--August 2006. Suspected cases met either the clinical or the biopsy criteria but not both. Hospital A staff members manually searched a logbook of dermatology biopsies to identify diagnoses consistent with NFD from January 2000 onward. Study investigators searched the hospital pathology database for diagnoses of NFD and potentially related diagnoses from the same period. Investigators searched for additional cases that would not have been identified at hospital A by contacting eight pathology referral centers in St. Louis and requesting information on all patients who had NFD diagnosed since January 2000. Demographics, comorbid conditions, and medication data for case-patients and controls were collected from hospital A inpatient and outpatient medical records, which included information from hospital A admissions (including emergency department visits), outpatient dialysis and other clinic visits, and laboratory and radiology studies performed in the hospital A system. The maximum erythropoietin (epoetin alfa) dose received during the preceding 6 months and the dose received at the time of disease detection (for case-patients) or match date (for controls) were classified as high or low relative to the median weekly dose received by all patients in the study. Continuous variables were compared using the Wilcoxon rank-sum test, and categorical variables were compared using a chi-square test or Fisher's exact test. Matched univariate odds ratios (ORs) were calculated. After adjusting for clinically relevant variables determined to be associated within the univariate analysis, multivariable ORs were calculated using a conditional logistic regression model. The case-control study included confirmed cases from hospital A. Three controls per case-patient were selected randomly from a group of patients who were treated in the same hospital A dialysis clinic or treatment center on the same day that a case was diagnosed. These matched controls were required to have received dialysis for at least 4 weeks or to have had renal insufficiency (serum creatinine >2.5 mg/dL) for at least 6 months preceding their match date. Only case-patients and controls with medical record information available for at least 3 of the 6 months preceding the match date were included. Twenty-eight cases were identified at hospital A during December 2002--August 2006, including 25 confirmed and three suspected cases (Figure). Five additional patients from St. Louis with NFD outside of hospital A were identified during the study period; however, minimal information was available for these patients, and they were excluded. Among the 19 confirmed case-patients at hospital A who met criteria for inclusion in the case-control study, the median age was 50 years (range: 21--67), and 10 (53%) were male. The median number of months on dialysis was 30 (range: 0.1--192 months). The primary type of dialysis received in the 6 months preceding disease detection was hemodialysis for 11 (58%) of the 19 case-patients and peritoneal dialysis for six (32%) case-patients. Two of the 19 case-patients had acute renal failure and received dialysis only for a brief time (4 days for one patient, 45 days for the other) during the 6 months preceding disease diagnosis. The clinical sites at which NFD was first detected were hospital A during inpatient hospitalization for 13 (68%) case-patients, an outpatient peritoneal dialysis clinic affilitated with hospital A for four (21%) case-patients, and an outpatient hemodialysis unit affiliated with hospital A for two (11%) case-patients. No significant differences were detected between case-patients (n = 19) and matched controls (n = 57) regarding sex, number of months since first dialysis, primary type of dialysis received, inpatient hospitalization days in the preceding year, and presence of diabetes mellitus (Table 1). Significant differences were detected in median age, history of deep venous thrombosis (DVT), history of hypothyroidism, and presence of dependent edema. In univariate-matched analysis, exposure to gadolinium-containing contrast agents during the preceding 6 months or preceding year was more common among case-patients than controls (Table 2). The presence of dependent edema, history of DVT, and history of hypothyroidism also were associated with NFD. Although the associations were not statistically significant, case-patients were more likely than controls to have received a high dose (>18,000 U/week) of erythropoietin at the time of disease detection and a high maximum dose (>30,000 U/week) of erythropoietin in the preceding 6 months. After adjusting for age, presence of dependent edema, history of DVT, and history of hypothyroidism, only exposure to gadolinium-containing contrast agents during the preceding 6 months or preceding year remained statistically significant. Five case-patients had no identified gadolinium exposure within 1 year preceding NFD diagnosis. However, of these, four had gadolinium exposure from 16 to 68 months preceding diagnosis; the fifth patient had no evidence of gadolinium exposure. Among case-patients (n = 14) and controls (n = 14) with gadolinium-containing contrast exposure in the preceding year, case-patients were more likely to have received peritoneal dialysis as their primary type of dialysis in the preceding 6 months (36% versus 0%) and had a longer median time on dialysis (27 months versus 10 months). Thirteen patients (nine case-patients, four controls) had multiple gadolinium-containing contrast exposures during the preceding year. The NFD attack rate estimated for persons undergoing outpatient chronic dialysis in the hospital A system for the 4 years in which cases were identified was 4.6 cases per 100 peritoneal dialysis patients and 0.61 cases per 100 hemodialysis patients. Reported by: S Cheng, MD, L Abramova, MD, Washington Univ School of Medicine, St. Louis; G Saab, MD, Univ of Missouri School of Medicine, Columbia; G Turabelidze, MD, Missouri Dept of Health and Senior Svcs. P Patel, MD, M Arduino, DrPH, T Hess, Div of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases (proposed); A Kallen, MD, M Jhung, MD, EIS officers, CDC. Editorial Note:NFD was first identified in 1997 as a fibrotic disorder of the skin in patients with renal failure (1). Since then, systemic involvement has been described in some patients with NFD, resulting in use of the term nephrogenic systemic fibrosis (NSF); NFD and NSF have been used to describe the same condition (3). No clear etiology has been established for NFD, and little is known about its pathogenesis or natural history. This report describes the largest geographic cluster of NFD that has been identified and provides evidence that exposure to a gadolinium-containing contrast agent is a risk factor for the development of the disease. Although risk factors for NFD have not been studied extensively, possible correlations with severity of renal failure, thrombotic episodes, edema, and vascular procedures have been reported (2,4). Recently, medication exposures such as erythropoietin and gadolinium-containing contrast agents have been identified as potential risk factors for NFD (5,6). In May 2006, the Danish Medicines Agency reported 25 cases of NFD diagnosed in Europe among patients with recent exposure to gadolinium-containing contrast. In response, the Food and Drug Administration (FDA) issued a public health advisory in June 2006 regarding the use of these contrast agents in patients with renal failure (7). As of December 25, 2006, the FDA MedWatch system had received 90 reports of NFD possibly related to gadolinium-containing contrast agents. Intravenously administered contrast agents are used routinely for MRI studies; the contrast agents contain gadolinium (a paramagnetic heavy metal), which is bound to a chelating agent. The mechanism for possible gadolinium-associated NFD is unknown; however, one hypothesis is that the gadolinium ions might dissociate from the chelate and result in a fibrotic reaction (5). Five gadolinium-based contrast agents are available in the United States; the first was approved for use in 1988 (7). Adverse events associated with these agents typically are minor (e.g., nausea); severe effects such as allergic reactions or tissue necrosis as a result of extravasation are rare. In addition, gadolinium-containing contrast agents are believed to be less nephrotoxic than iodinated contrast agents used for computed tomography (CT) imaging (8). Excretion of gadolinium-containing contrast agents primarily occurs renally; the amount of contrast eliminated from the body after dialysis has not been well-evaluated. Two studies suggest that 65%--78% of gadolinium-containing contrast might be cleared after one hemodialysis session and 98% after three sessions (9,10). Peritoneal dialysis might achieve less effective gadolinium-contrast clearance than hemodialysis. In one study, 69% of total gadolinium-containing contrast was excreted after 22 days in patients undergoing continuous ambulatory peritoneal dialysis (9). Delayed clearance might prolong the duration of gadolinium-containing contrast exposure among patients undergoing peritoneal dialysis. However, patients undergoing peritoneal dialysis have not been previously reported to be at higher risk for NFD than patients undergoing hemodialysis. The chronic peritoneal dialysis outpatients in this investigation had higher estimated NFD attack rates than chronic hemodialysis outpatients. No controls who had gadolinium-containing contrast exposure underwent primarily peritoneal dialysis. The number of cases identified at hospital A decreased during the second and third quarters of 2006 (Figure), and the reason for this decrease is unclear. Because NFD was not recognized at hospital A until late 2002, initially identified cases likely represented both incident (new) and prevalent (existing) cases; the decline might represent the subsequently smaller number of remaining prevalent cases that had not been identified. Although hospital A instituted changes such as limiting the use of gadolinium-containing contrast agents in patients with renal failure, these changes were initiated shortly before the investigation began and are unlikely to account completely for the decline. The findings in this report are subject to at least two limitations. First, NFD is a rare condition. Even though the data in this report represent the largest cluster of NFD cases identified to date, the small sample size of the case-control study might have limited the power to demonstrate statistically significant associations for variables other than exposure to gadolinium-containing contrast agents. Second, the date of disease diagnosis was used instead of date of disease onset; the actual date of disease onset is unknown. To identify exposures that preceded the actual date of disease onset, exposures as early as 1 year before the date of diagnosis were included. This might have resulted in the inclusion of gadolinium exposures that were not related to the development of NFD. When possible, use of gadolinium-containing contrast agents should be avoided in patients with advanced renal failure, particularly in patients who are undergoing peritoneal dialysis. Depending on the indication for imaging, other radiologic modalities (e.g., ultrasound and CT) might be acceptable substitutes in certain situations. If gadolinium-containing contrast is medically necessary, prompt hemodialysis after contrast administration to facilitate clearance of the contrast might be reasonable for patients who have established hemodialysis access; however, the effectiveness of this strategy in reducing the risk for NFD development or progression is unknown. Among patients with no other indication for chronic or acute hemodialysis, the risks of establishing hemodialysis access should be weighed against theoretical benefits of hemodialysis after gadolinium-containing contrast administration. CDC and FDA are collaborating to assess potential differences among gadolinium-containing contrast agents, including the associated risk for NFD and possible related factors. Additional studies are needed to assess the ability of peritoneal dialysis and hemodialysis to clear gadolinium-containing contrast agents and to clarify the mechanism by which use of gadolinium or chelating agents might result in NFD. Clinicians who treat patients with renal disease should be aware of the risk for NFD and consider the diagnosis in patients with characteristic skin lesions. Suspected adverse drug events should be reported to FDA via the MedWatch program by phone (1-800-FDA-1088), by fax (1-800-FDA-0178), or online (http://www.fda.gov/medwatch/index.html). Acknowledgments The findings in this report are based, in part, on contributions by S Cowper, MD, Yale Univ School of Medicine, New Haven, Connecticut; C Kwoh, MD, D Berk, MD, Washington Univ School of Medicine, St. Louis, Missouri; DG Kleinbaum, PhD, Dept of Epidemiology, Rollins School of Public Health at Emory Univ, Atlanta; R Wang, DO, S Pappas, PhD, J Jarrett, MS, Div of Laboratory Sciences, National Center for Environmental Health, and J Guarner, MD, Div of Viral and Rickettsial Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases (proposed), CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 2/22/2007
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|